HFREF with severe PAH
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case Presentation:
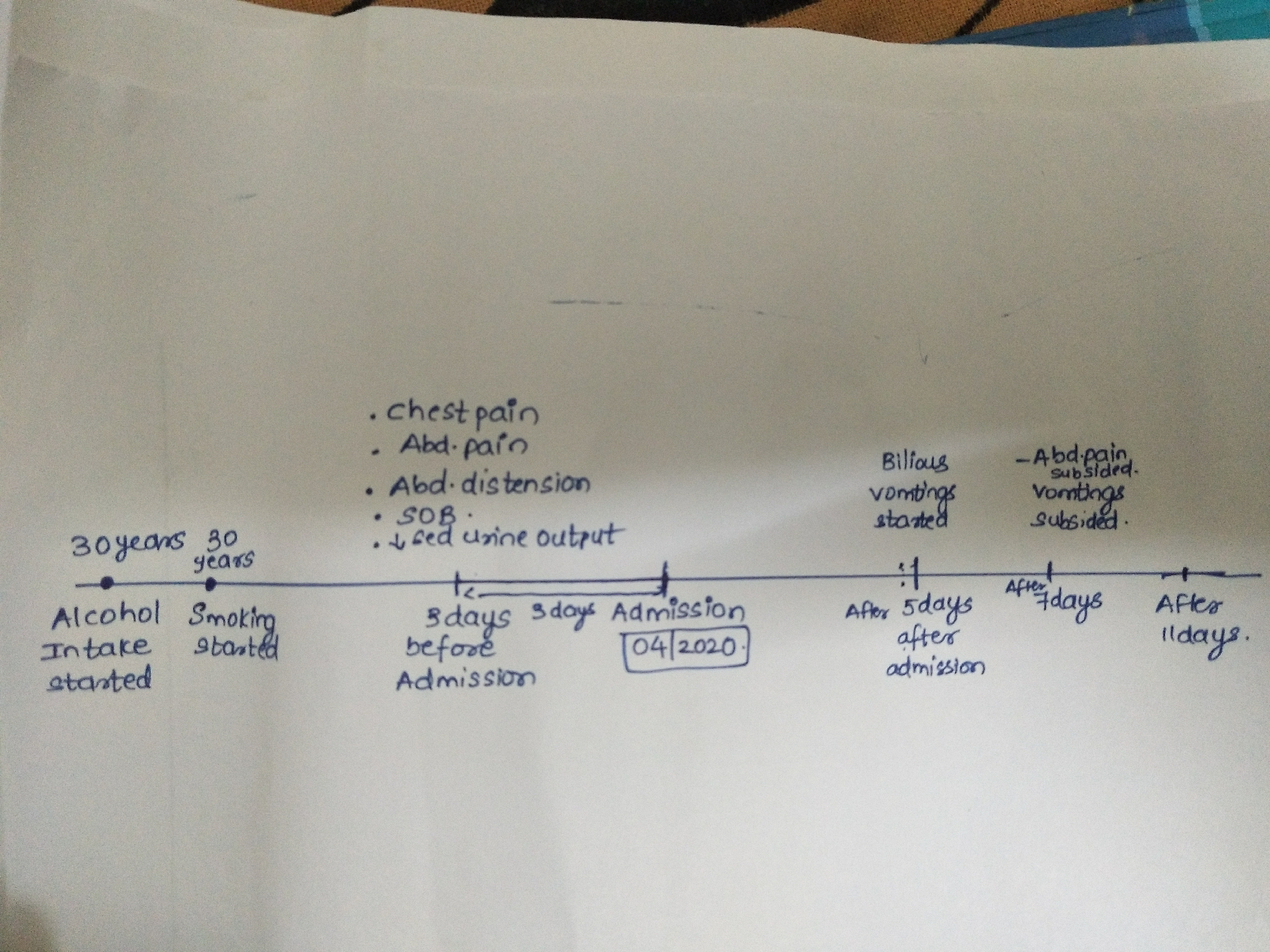
52 year old woman presented to the casualty with the complaints of
Dyspnea on exertion since 4 months
Bilateral pedal edema since 4 months
Abdominal distension since 4 months
Unable to pass flatus since 3 days
Passage of hard stools since 3 days
She got married to a cook when she was 15 years old.
She has 2 children - her son who is 35 years old , works at a hostel and has 4 girls and her daughter is 32 years old and is a housewife. She had to undergo LSCS for both her deliveries as she was told that she had a big baby. She underwent tubectomy 32 years ago.
Her husband met with an accident 25years back and since then he cannot walk without support, she was the only financial support for her kids, she started working at a hostel where she used to cook on a biogas stove.
4 years back, one fine morning she experienced giddiness after which she was taken to the hospital and got diagnosed to be hypertensive. She was put on Tab Cilnidipine 5mg which she has been taking religiously since then.
4months back one day she developed fever with chills and subsequently noticed yellowish discolouration of eyes after which she took herbal medications. Few days after which she developed dyspnea which was sudden in onset even at rest, further aggravated on walking and subsequently she developed bilateral pedal edema extending to her knees followed by abdominal distension and facial puffiness. She was taken to a local hospital where in she was told she had heart failure and was even told that she had water accumulated around her heart and was also detected to be a diabetic. She got diagnosed with heart failure with reduced ejection fraction (EF - 25%).She was put on Tab Dytor plus Twice daily, Tab Clopitab AV, Tab Cilnidipine 5 mg, Tab Glycomet M1 OD. Her symptoms were relieved with these medications but She stopped using medications after 2 months as she was tired of taking these medications everyday.
She says both her lower limbs have become swollen after she stopped using medications and even feels dyspneic after walking for a short distance of less than 100m. She has been finding it difficulty to pass flatus since 3 days.
On examination
Pallor +
Bilateral pedal edema +
CVS -
Apex beat present in the 6th ICS 4cms away from the Midclavicular line
Muffled S1,S2 +
R/S -
Bilateral infrascapular fine crepts +
Reduced breath sounds in bilateral IAA
P/A - soft, non tender, no orgsnomegaly
Bowel sounds +
CNS examination:
Higher mental functions
1) speech - slurred
2) memory - a) recent +
b) immediate +
c) remote +
3) orientation to time, place and person present.
Cranial Nerve examination :
1CN olfaction - intact
2CN visual acuity, hand movements and colour vision intact
3,4,6 CN extraocular movements normal
5CN sensations on face present, mastication present, jaw jerk present
7 CN no dropping of eyelids, absence of frowning, deviation of mouth to right side, nasolabial fold wrinkling, taste intact
8 CN tuning fork tests normal
CN 9,10,11 intact
CN 12 deviation of mouth to left side
Motor examination :
Right. Left.
1) Bulk UL Proximal N. N
Distal N. N
LL proximal. N. N
Distal. N. N
2)Tone. UL proximal N. N
Distal. N. Increased
LL proximal. N. Increased Distal. N. Increased
3)power UL proximal 4/5. 4/5
Distal. 4/5. 4/5
LL proximal. 4/5. 4/5
Distal. 4/5. 4/5
Hand grip. 100. 80
4) Reflexes. Right. Left
Biceps. ++ ++
Triceps. ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. 0 0
Plantar. Extensor. Flexor
5) superficial reflexes
Cornea, conjunctiva and abdominal reflexes intact
Sensory examination:
1)Proprioception, fine touch, vibration and joint position - intact
2)anterior spinothalamic tract intact
No abnormality detected in cortical and cerebellar functions
Normal gait
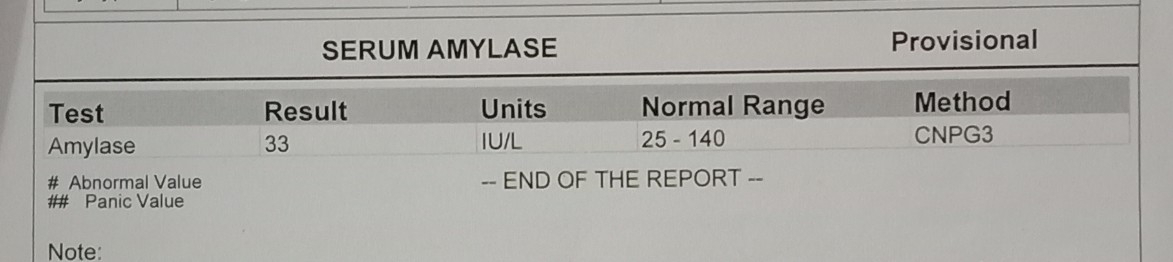
Investigations :







Diagnosis :
HFREF with severe PAH
?CVA - UMNL type with facial palsy and 12th CN involvement and B/L pleural effusion.
K/c/o HTN, type 2 DM
Treatment :
1) propped up position
2) salt restriction <2.4g/day
3) fluid restriction <1lit/day
4) inj ladies 40mg iv bd
5) tab Tells 40mg PO OD
6) tab Glycomet GP-1 PO OD
7) tab Neurobion forte PO OD
8) syp Lactulose 15ml PO H/S
9)tab ecosprin ax 75/20.1 mg PO H/S
10)strict I/O charting
11) BP, PR, Temperature charting 4th hourly.