bimonthly assessment for November 2020
Inferior wall MI(normal ecg and echo)
Acute pancreatitis(radiation to the back)-usg finding and elevated serum amylase level
Perforated peptic ulcer
Causes of acute pancreatitis-harrison pg no 2348
Gall stones :https://gi.org/topics/gallstone-pancreatitis/
This occurs at the level of the sphincter of Oddi, a round muscle located at the opening of the bile duct into the small intestine. If a stone from the gallbladder should travel down the common bile duct and get stuck at the sphincter, it blocks outflow of all material from the liver and pancreas. This results in inflammation of the pancreas that can be quite severe.
2)sob- acidosis due to renal failure
? Ards secondary to sepsis/pancreatitis
Pleural effusion due to acute pancreatitis
3)decreased urine output-pre renal Aki secondary to volume loss(oliguric)
3rd space loss due to pancreatitis
Sepsis induced aki
4) abdominal distention with constipation and nausea
Secondary to paralytic ileus
B) pharmacological interventions
https://link.springer.com/article/10.1007/s00534-005-1050-8
1)fluid replacement
Increased vascular permeability in acute pancreatitis causes the loss of intravenous fluid and reduces plasma volume. In severe cases, in patients with massive ascites, pleural effusion, and retroperitoneal and mesenteric edema, circulating plasma volume decreases markedly. Hypovolemia may lead to shock and acute renal failure, and, because hypovolemic shock may impair the pancreatic microcirculation and promote pancreatic ischemia and necrosis, restoration and maintenance of plasma volume is crucial in severe acute pancreatitis.
2) antibiotics
On the other hand, a placebo-controlled, double-blind trial of ciprofloxacin + metronidazole in patients with predicted severe acute pancreatitis showed that prophylactic administration of these antibiotics did not prevent pancreatic infection (Level 1b).
3)analgesics
4) nebulization in view of b/l wheeze secondary to ?copd
5)diuretics for decreased urine output due to renal failure
Non pharmacological interventions
1)nill per mouth
https://pubmed.ncbi.nlm.nih.gov/27107634/
2)ryles tube catheterisation
3)oxygenation
Case-2
https://aakansharaj.blogspot.com/2020/11/55-year-old-male-with-anemia.html?m=1
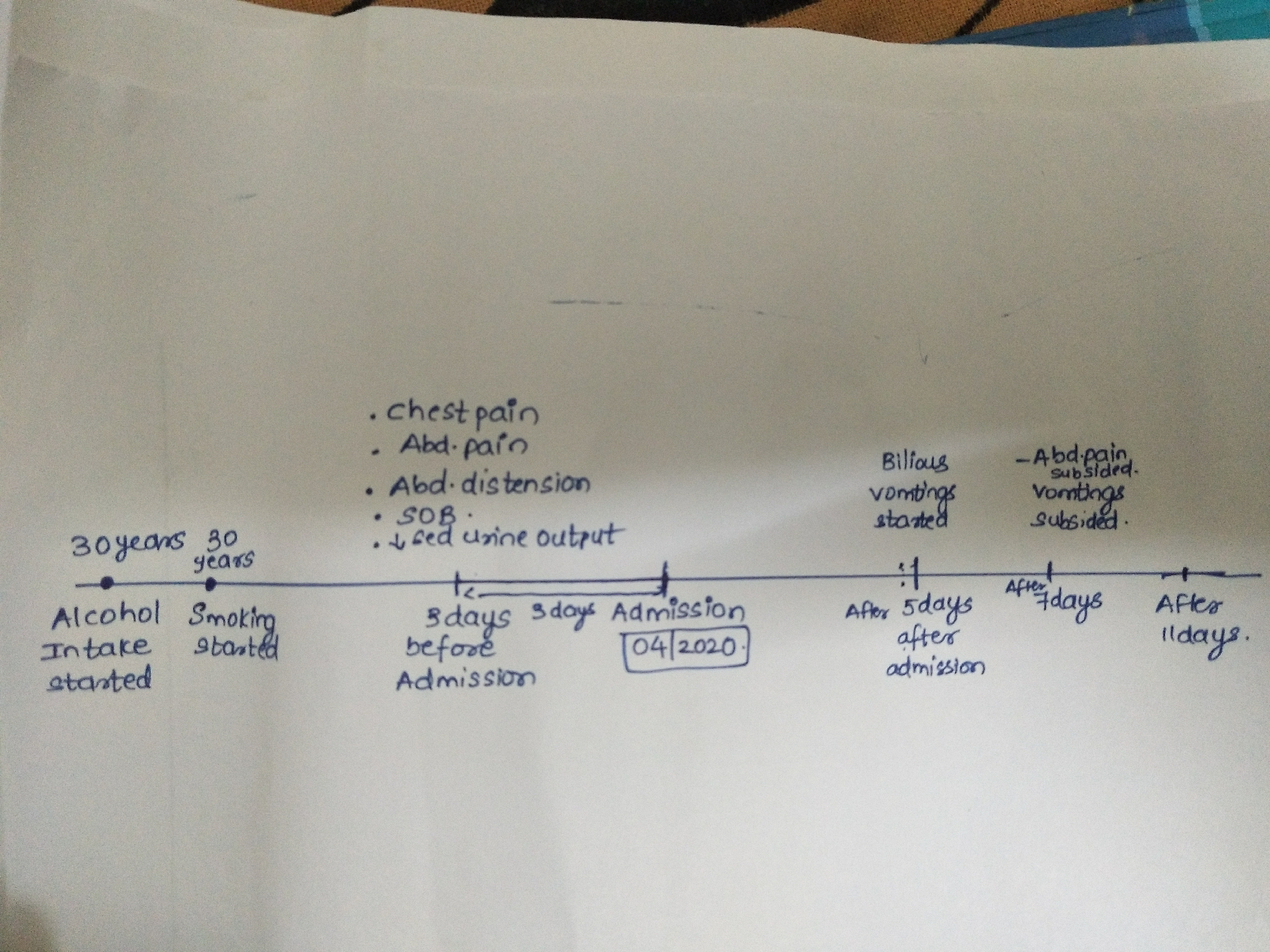
A) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
ANATOMICAL LOCATIONS WITH ETIOLOGY:
BONE MARROW
Etiology: Multiple myeloma
KIDNEYS
Etiology: AKI due to multiple myeloma
HEMATOLOGICAL (ANEMIA)
Etiology: secondary to multiple myeloma
LUNGS
Etiology: Tuberculosis (Increased susceptibility to infections)
TIMELINE OF EVENTS:
Alcohol & smoking (35 years)
!
Stopped alcohol (4 years)
!
Fever , generalised weakness & anemia - 2 units blood transfusion (1.5 years)
!
Stopped smoking (4 months)
!
Low grade fever , generalized weakness , headache , neck pain , loss of appetite , weight loss (2 months)
!
Cough & SOB (2 weeks)
!
Vomiting & pain abdomen (2 days)
OUTCOME:
Some symptomatic relief and referred to higher centre in need for oncologist
B) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
PHARMACOLOGIC :
1.ANTIBIOTICS : For underlying infection (Azithromycin for ?Atypical pneumonia)
2.ATT : For TB
3.SEVELAMER : For hyperphosphatemia
4.FEBUXOSTAT : For hyperuricemia
5.PRBC transfusion for anemia
Case-3
http://nithishaavula.blogspot.com/2020/11/51-yr-old-male-with-hfref.html?m=1
A) Where are the different anatomical locations of the patient's problems and what are the different etiologic possibilities for them? Please chart out the sequence of events timeline between the manifestations of each of these problems and current outcomes.
1.Diabetes and hypertension causing macrovasuclar and microvascular dysfunction
2.Heart failure with reduced ejection fraction
LVF due to hypertension
Leading to PAH
PAH causing right heart failure
3.Atrial fibrillation :heart failure ,diabetic and hypertension are also risk factors for AF.
4) Due to AF - there is formation and dislodgement of thrombus , leading to stroke in this patient.
5.seizures in this patient is again due to stroke .
(Infarct in right frontal lobe ).
SEQUENCE OF EVENTS

b) What are the pharmacological and non pharmacological interventions used in the management of this patient and what are the efficacy of each one of them?
Preload reducing agents - Diuretics (only if symptomatic)
Afterload reducing agents - vaso dilators ,ace inhibitors and arb
Beta blockers for preventing cardiac remodeling and reduce mortality.
https://pmj.bmj.com/content/79/937/634
Antiepileptics ( known case of epilepsy)
Insulin for glycemic control in diabetes.
Non pharmacological interventions
Salt and fluid restriction
https://pubmed.ncbi.nlm.nih.gov/23787719/
Individualized salt and fluid restriction can improve signs and symptoms of CHF
Case 4
https://nairaditya97.blogspot.com/2020/11/31-yr-old-male-with-bl-pedal-edema-with.html?m=1
1)heart(rt and left)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5851725/
Wet beriberi is one of the clinical syndromes associated with thiamine deficiency. Thiamine, in its phosphorylated form thiamine pyrophosphate (TPP), is the precursor for the cofactor of both pyruvate dehydrogenase and alpha-ketoglutarate dehydrogenase, which are both key enzymes of the Krebs cycle. The Krebs cycle is an essential part of aerobic glucose metabolism. A decrease in the activity of these 2 enzymes due to thiamine deficiency may lead to the tissue accumulation of pyruvate and lactate.[1] Moreover, the accumulation of pyruvate and lactate decreases peripheral resistance and increases venous blood flow, increasing the cardiac preload. Increased preload and myocardial dysfunction ultimately leads to congestive heart failure.
https://www.medindia.net/patients/patientinfo/beriberi-disease.htm
Other conditions cause beriberi include:
- Excessive alcohol usage, which results in inadequate intake in the diet as well as prevents the body from absorbing and storing vitamin B1.
- Genetic beriberi, which is an inherited condition where people lose the ability to absorb thiamine from foods. Symptoms usually present during adulthood.
- Pregnancy; pregnant women often present with vitamin B1 deficiency. Breastfeeding infants can suffer from vitamin B1 deficiency if the mother is deficient.
- People with endocrine disorders like hyperthyroidism who require extra vitamin B1.
- Chronic liver disease, which prevents the body from absorbing sufficient vitamin B1.
- Kidney dialysis, which leads to a loss of vitamin B1.
- A prolonged bout of diarrhea, which also leads to a loss of vitamin B1.

1) pharmacological interventions
Diuretics
Thiamine
2)non pharmacological interventions
Salt and fluid restriction

